Dr Gul Deniz Salali (Lecturer in Evolutionary Anthropology/Medicine, UCL Anthropology) details her findings from a new survey on behavioural responses to COVID-19, revealing why many Europeans may be hesitant to get a vaccine.
Another piece detailing Salali’s findings appeared this month on The Conversation UK.
News of a COVID-19 vaccine with 90% efficacy has generated much enthusiasm around the world. Vaccine development itself, however, will not be enough to stop the virus–a sufficient amount of people will need to be vaccinated for widespread immunity. Vaccine hesitancy (delay in acceptance or refusal of vaccines) has been on the rise across the globe and was listed in 2019 as one of the top ten threats to global health by WHO. The recent outbreak of measles in the UK and Europe, for instance, is largely caused by vaccine hesitancy as a result of misinformation about the MMR vaccine.
The question of why we find certain beliefs and information more attractive than others has always interested me. Since the start of the pandemic, I observed many people discussing different theories on the origin of the novel coronavirus. This is why my social psychologist colleague, Mete Sefa Uysal from Dokuz Eylul University in Turkey, and I have decided to conduct a study on people’s opinions on the origin of the novel coronavirus and the potential COVID-19 vaccine. We asked 3936 participants in Turkey, and 1088 in the UK, questions about their willingness to vaccinate for a COVID-19 vaccine and about their beliefs on the origin of the virus (natural (i.e. originated in wildlife) / artificial (i.e. originated in a laboratory) / not sure).
Our results, published in Psychological Medicine, showed that about one in three people (31%) in Turkey and one in seven (14%) in the UK are ‘hesitant’ about a COVID-19 vaccine. In both countries, 3% of the participants rejected a COVID-19 vaccine. To achieve herd immunity for a disease like COVID-19, an estimated 50 to 75% of the population needs to be vaccinated. Given that, the level of hesitancy for the COVID-19 vaccine we found in our study is concerning, especially for Turkey.
Why are people hesitant for a potential COVID-19 vaccine?
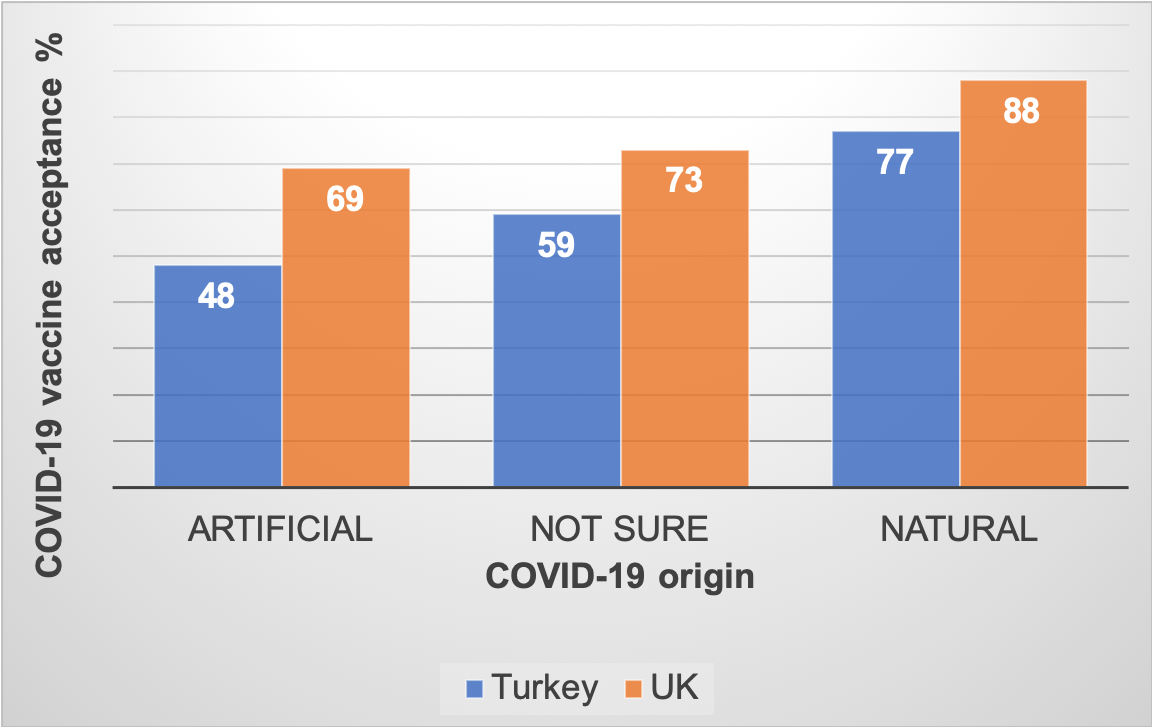
We examined the factors associated with acceptance of a COVID-19 vaccine. One of the key factors that explained the probability of vaccine acceptance was a person’s belief on the origin of the novel coronavirus. Only 48% of the people in Turkey and 69% in the UK who thought the virus origin to be artificial accepted COVID-19 vaccination. Vaccine acceptance rates rose to 77% in Turkey and 88% in the UK if a person believed that the virus originated naturally in wildlife.
Research to date has shown that COVID-19 had a natural origin. Nevertheless, many conspiracies on the origin of the novel coronavirus have emerged. Our results reinforce previous findings showing an association between conspiratorial worldview and vaccine hesitancy.
But why do people believe in conspiracies which render them more hesitant about vaccinations? People who believe in one conspiracy are more likely to believe in others. Moreover, conspiratorial worldview is not only associated with vaccine hesitancy, but with a general rejection of scientific propositions such as the wildlife origin of the novel coronavirus. Therefore, a better question to ask is: “Why do people reject science?” Our evolved cognitive biases may explain why many people find it hard to accept scientific explanations.
One such bias is the intuitive bias: we find beliefs that are in line with our intuitions easier to understand and remember. Many scientific facts are not intuitive at all. Take, for example, the discovery of Earth being round. This took a long time to be accepted because it was not in line with our intuitions. Likewise, vaccination is counter-intuitive: an anti-vaccination message saying “injecting a dose of weakened microorganism into one’s body is harmful” is probably more intuitive than the message that it will be helpful.
Moreover, our minds have evolved to make the least costly decision when there is uncertainty. This is why, when people face a choice between taking a specific action or doing nothing, they sometimes prefer to do nothing. This cognitive bias, called the omission bias, may kick in when people make vaccination decisions. We still have lots of unknowns about the novel coronavirus and this uncertainty may increase vaccine hesitancy.
Now, you may be asking if scientists do not have these biases themselves. Yes, we all do. But the scientific worldview is a product of a slow, cumulative process where each discovery is built on the collective work of the previous scientists and subject to careful “selection”. This cumulative progress of science allows us to surpass the limitations of individual cognitive capacities.
Men and people with higher pandemic-related worries are more likely to vaccinate for COVID-19
Other behavioural and demographic factors were associated with COVID-19 vaccine acceptance in our survey. For instance, we asked participants about the level of their anxieties related to the pandemic, such as being more worried about catching or passing on the virus. A one-point increase in their pandemic-related anxiety score (on a scale of one to four) increased the odds of vaccine acceptance by 36%.
As the prominent evolutionary psychiatrist Randolph Nesse writes in his recent book, “Good Reasons for Bad Feelings”, the emotions can be seen as detectors helping us to avoid death or promote reproduction. In this sense, anxiety acts like a smoke detector. Our worries are often unnecessary, just like a smoke detector that goes off unnecessarily when you are cooking. You would still want to keep your smoke detector since one “right” alarm could be lifesaving. The positive correlation between COVID-19 related anxiety and vaccine acceptance can be rooted in the adaptive function of anxiety in decreasing mortality risk.
Compared to women, men in Turkey were more likely to accept a COVID-19 vaccine and believe in the natural origin of the virus. Another recent cross-cultural study has shown increased rates of COVID-19 vaccine acceptance in men. Because women are more likely to make healthcare decisions for their children, they may also be more likely to seek out information about vaccines and be exposed to online anti-vaccination content. Moreover, women score higher on disgust sensitivity which is associated with vaccine hesitancy.
Cross-cultural differences in vaccine hesitancy
Cross-cultural studies on vaccine hesitancy are necessary in an ever-connected world, as each country’s success in slowing infections is a benefit to other countries.
According to WHO measles surveillance data for 2019, the European region has recorded a 300% increase in measles cases. The 2018 Wellcome Global Monitor report indicates that in high-income regions there is less certainty about vaccine safety, with 59% of people in Western Europe “agreeing” that vaccines are safe, as opposed to 79% globally. According to a 2019 survey, one in 30 sets of parents in the UK opposed all vaccinations, and 7.4% of parents reported being against compulsory vaccination. Among Western European countries, France is the highest in vaccine scepticism with one in three people disagreeing that vaccines are safe. The level of trust in public health authorities in France and Italy are the lowest among the Western European countries. In recent years, vaccine hesitancy has risen sharply in Turkey, with the number of families signing a vaccine rejection form increasing from 183 in 2011 to 12,000 in 2016. Consequently, Turkey has seen a rise in confirmed measles cases from 9 in 2016 to 2890 in 2019. Worldwide, Eastern European countries are the least likely to agree that vaccines are effective and safe, with 24% of people surveyed in Russia strongly disagreeing with the statement that vaccines are safe.
Why do we observe different levels of vaccine hesitancy across countries? Contributing to the observed difference in COVID-19 vaccine hesitancy between UK and Turkey, more participants in the UK believed in the natural origin of the virus (54% in Turkey, 63% in the UK), while18% in Turkey and 12% in the UK thought the origin to be artificial. Some country-level differences might have contributed to these observed differences. For example, we asked participants (who are younger than 75) what they thought their probability of living up to 75 or more was on a scale of 0-100. The mean perceived life expectancy was much lower in Turkey than in the UK (57 vs 75). Individuals in countries with lower life expectancy (i.e. increased mortality risk) may exhibit increased threat perception and out-group mistrust, promoting a conspiratorial worldview. Moreover, the mean financial satisfaction score was lower in Turkey (from a scale of 0-100: 67 in the UK vs 48 in Turkey), a significant predictor explaining the virus origin beliefs in both countries.
How can we combat vaccine hesitancy?
People tend to cherry-pick information that is in line with their intuitions, and this process of “motivated reasoning” amplifies negative attitudes toward vaccination. Researchers have also acknowledged the ineffectiveness of trying to reduce conspiratorial thinking simply by challenging people’s worldviews.
Nevertheless, understanding the cognitive mechanisms that motivate people to accept and reject vaccines should be our first step toward planning more effective strategies to promote vaccination uptake. Our study findings point at a concerning level of COVID-19 vaccine hesitancy, especially in Turkey. Many studies like ours indicate that one of the strongest predictors of vaccine hesitancy is belief in conspiracies and the general rejection of scientific explanations associated with this. Therefore, we need to think more about how to communicate scientific findings on the origin of the novel coronavirus and the safety of a COVID-19 vaccine more effectively. It may also be more effective to emphasise the risk of disease (not only individual risk but risk to the others in the community) rather than merely providing scientific facts.
Photo by National Cancer Institute on Unsplash
Note: The views expressed in this post are those of the author, and not of the UCL European Institute, nor of UCL.





Leave a comment